Pericarditis is the Most Likely Caused by a Continuous Murmur
Acute pericarditis is the most common disease state affecting the pericardium. Most cases of acute pericarditis are idiopathic or have a viral etiology.1,2 Other potential etiologies include bacterial and fungal infections, rheumatologic conditions, inflammatory bowel disease, drug reactions, malignancies, uremia, pregnancy and immunologic disorders (Table 1).1,3–5 Patients typically complain of sharp central chest pain that worsens with recumbency and is relieved by leaning forward. The pain associated with acute pericarditis may be pleuritic in nature and may radiate to the ridge of the trapezius, a sign very specific for pericardial inflammation.6
Physical examination may reveal the pathognomonic finding for pericarditis: the pericardial friction rub. Classically, this rub occurs in three phases corresponding with atrial systole, ventricular systole and ventricular diastole. However, it is uncommon for all three phases to be heard clinically and, at times, the rub may be evanescent.2 The friction rub is best appreciated by firmly applying the diaphragm to the left lower sternal border with the patient leaning forward after an exhalation.
The electrocardiogram (ECG) is very useful in the diagnosis of acute pericarditis. Characteristic manifestations of acute pericarditis on ECG most commonly include diffuse ST-segment elevation. However, other conditions may have ECG features similar to those of acute pericarditis. These conditions most commonly include acute myocardial infarction and early repolarization. Since these and other conditions require distinctly different treatments, physicians should be able to recognize the typical manifestations of acute pericarditis. This article reviews some of the common ECG findings associated with acute pericarditis as well as criteria to differentiate acute pericarditis from other conditions.
Illustrative Case
A previously healthy 52-year-old man presented to the emergency department with a history of sharp, pleuritic central chest pain occurring over the past several hours. The pain began at rest, was exacerbated in the supine position and was relieved by leaning forward. There was no history of radiation of the pain, dyspnea, diaphoresis, palpitations, vomiting, or chills or fever. He had no prior history of pain or any chest trauma. A few weeks previously, he had noted a sore throat without other symptoms. He had no previous medical problems and took no medications. He did not smoke, consume alcohol or use illicit drugs. He had no known risk factors for human immunodeficiency virus infection. There was no family history of heart disease or collagen vascular disease.
The patient's pulse rate was 80 per minute, his respiration rate was 14 per minute, his blood pressure was 132/80 mm Hg, and his temperature was 36.5°C (97.8°F). There was no pulsus paradoxus or jugular venous distention. Cardiac examination revealed a regular rate and rhythm without murmurs; however, a two-phase friction rub was heard at the left lower sternal border. The remainder of the physical examination was normal.
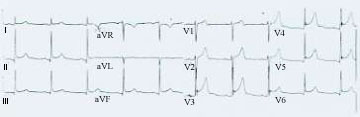
The following laboratory results were normal: blood urea nitrogen, creatinine, electrolytes, liver function tests, hemoglobin mass concentration, and white blood cell count. The erythrocyte sedimentation rate was 22 mm per hour, and the antinuclear antibody test was negative. A chest radiograph and echocardiogram were normal. The ECG revealed diffuse concave-upward ST-segment elevation with PR depression (Figure 1). A diagnosis of acute pericarditis was established, with the most likely etiology being either idiopathic or postviral. Viral serologies were not performed. The patient was treated with aspirin, 650 mg every six hours, and showed marked improvement by the following day. At the two-week follow-up visit, the patient was doing well.
Anatomy and Physiology of the Pericardium
The pericardium consists of an outer fibrous layer called the parietal pericardium and an inner serosal membrane overlying the epicardial surface called the visceral pericardium. Between these layers is a potential space normally containing approximately 20 mL of fluid, an ultrafiltrate of plasma.3,7 The majority of the parietal pericardium is composed of collagen fibrils arranged similar to an accordian, enhancing the elastic properties of the structure. On the ultrastructural level, the pericardium contains numerous villi and cilia that enhance fluid resorption and facilitate movement of pericardial surfaces over one another. Important functions of the pericardium include limiting acute distention of the heart, especially in states of volume overload, maintaining the heart in an optimal shape and position, and acting as a buttress against inflammation to prevent it from spreading to adjacent structures.3,8
Classic acute or "dry" pericarditis usually results in deposition of a fibrinous material with a characteristic "bread-and-butter" appearance likened to pulling two pieces of buttered bread apart. The vascularity of the pericardium is increased, which may impart a gross red appearance with diffuse fibrin deposition and neutrophils present on microscopic examination.9 It is this inflammation that creates the characteristic friction rub heard on auscultation, which has been described as being "like the squeak of leather on a new saddle under a rider, or grating in the knee joint on moving the patella over the femoral condyles."6
Electrocardiographic Manifestations
The ECG is useful in the diagnosis of acute pericarditis, with abnormalities found in approximately 90 percent of cases. Changes on ECG classically occur in four stages (Table 2).9,10 Not all cases of pericarditis include each of these four stages. In fact, all four stages are present in only 50 percent of patients or less. Stage I typically occurs during the first few days of pericardial inflammation and is mainly characterized by diffuse ST-segment elevation. This stage may last up to two weeks. Stage II is characterized by return of the ST segments to baseline and flattening of the T wave and may last from days to several weeks. Stage III usually begins at the end of the second or third week and is characterized by inversion of the T waves in the opposite direction of the ST segment; this stage may last several weeks. Stage IV represents the gradual resolution of the T-wave changes and may last up to three months.11
The most sensitive ECG change characteristic of acute pericarditis is ST-segment elevation, which reflects the abnormal repolarization that develops secondary to pericardial inflammation. There may also be ST-segment depression in leads aVR and V1. Typically, there are no changes during depolarization, so in the absence of underlying cardiac disease, the P wave and QRS complexes are normal.2 Depression of the PR segment is very specific of acute pericarditis and is attributed to subepicardial atrial injury and occurs in all leads except aVR and V1. These leads may exhibit PR-segment elevation.2,11,12
The pattern of ST-segment elevation is important in the diagnosis of acute pericarditis. The ST-segment elevation that occurs during acute pericarditis is usually "concave," compared with the "convex" appearance of the ST segment that occurs during the acute injury stage of a myocardial infarction. Another important feature of acute pericarditis is the widespread ST-segment elevation not corresponding with any specific arterial territory, which usually occurs in association with acute myocardial infarction.2 Also, reciprocal changes are absent in acute pericarditis, although they are frequently found with acute myocardial infarction. The ST segments in acute pericarditis return to baseline in a few days and are followed by diffuse T-wave inversion, in conjunction with the ST segment at baseline.11
Another feature that may aid in differentiating acute pericarditis from acute myocardial infarction is the absence of Q waves and the absence of T-wave inversion at the time of ST-segment elevation, both of which classically occur with acute myocardial infarction.2 Loss of R-wave progression may occur with acute myocardial infarction, but this feature is not present with acute pericarditis. Low voltage (i.e., decreased amplitude of the QRS complex) may also be present. Arrhythmias are uncommon in acute pericarditis. In one large study,13 no arrhythmias occurred in patients without underlying cardiac disease.
Differential Diagnosis of Acute Pericarditis by ECG
Acute pericarditis exhibits characteristic changes on ECG that usually enable one to make the diagnosis readily. There are other conditions that the clinician needs to consider in the differential diagnosis of acute pericarditis by ECG (Table 3). However, findings on the history and physical examination and on laboratory assessment usually narrow the diagnostic possibilities. Two conditions that are commonly confused with acute pericarditis include acute myocardial infarction and early repolarization (Figure 2).
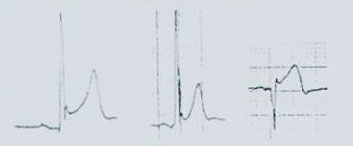
Early repolarization is a normal variant that occurs commonly in young males, especially blacks, and does not evolve with the stages of acute pericarditis.2 Early repolarization is distinguished by ST-segment elevation limited to the precordial leads, elevation of the ST segment in V1, an isoelectric ST segment in lead V6, notching of the terminal aspect of the QRS complex, and a shift to baseline of the ST segments with exercise.10,11
Another useful clue in differentiating acute pericarditis from early repolarization is the ST/T ratio in lead V6. This is calculated by dividing the millimeters of ST-segment elevation by the millimeters to the tallest point of the T wave. Each value is measured from the isoelectric point. An ST/T ratio of greater than 0.25 in lead V6 suggests acute pericarditis.10,14 Table 4 lists findings on ECG that are characteristic of acute pericarditis, acute myocardial infarction and early repolarization.
Follow-up
Most cases of acute idiopathic or viral pericarditis do not recur; however, acute pericarditis may recur if it is associated with an ongoing underlying illness such as an autoimmune disease or uremia. Symptoms usually subside within two weeks; however, up to 15 percent of patients may experience a recurrence in the first few months following the initial episode.1,5,15 On occasion, idiopathic acute pericarditis may recur several times but will rarely lead to effusion and cardiac tamponade or constrictive pericarditis necessitating pericardectomy.3 Typically, physicians should schedule a follow-up visit with these patients two weeks after the onset of their illness unless problems arise sooner. An ECG should be considered at four weeks, bearing in mind that residual T-wave inversion may be present for several weeks during stage III of acute pericarditis.1,5,10,15.
Source: https://www.aafp.org/pubs/afp/issues/1998/0215/p699.html
0 Response to "Pericarditis is the Most Likely Caused by a Continuous Murmur"
Post a Comment